Research
At the Center, we support all of our activities with sound evidence gathered through research. We collaborate with local and national experts to discover effective recovery oriented practices that can be readily applied. We seek to answer the questions that are relevant and important to every practitioner: what works best for who and why?
Current Research
Integrated Recovery Housing on Clinical Outcomes
- Tanya Freedland, MPS, LADC
- Jennifer Wiseman, MPS, LADC
- Julie Rohovit, Ph.D.
The Center for Practice Transformation was hired by Minnesota’s largest non-profit extended care addiction and mental healthcare treatment provider NUWAY® House, Inc. (NUWAY®) to study the effects of integrated recovery housing on clinical outcomes with the goal of providing data-driven care to people in recovery. The program evaluation, which began in 2019, is ongoing and has enrolled 5,000 participants over the course of the project. This study has provided a wealth of information, allowing NUWAY® to augment programming to better serve its clients using data collected and analyzed by CPT, an unbiased third-party. More and more, programs are required to demonstrate effectiveness using data-driven approaches. NUWAY® is serving as a model for programs in Minnesota and nationwide by engaging in scientifically sound research on clinical outcomes. View the latest news here.
Past Research
Provider Preparedness for Treatment of Co-occurring Disorders: Comparison of Social Workers and Alcohol and Drug Counselors
- Colleen Fisher, PhD
- Jennifer Simmelink McCleary
- Peter Dimock, MSW
- Julie Rohovit, PhD
Social workers and alcohol and drug counselors are the primary providers of mental health services for people with CODs and provide services in screening, diagnostic assessment, case management, treatment team supervision, and agency administration. Providers who are capable of providing high fidelity integrated treatment must have sufficient knowledge and training in both mental health and substance use. While social workers and alcohol and drug counselors provide most services for individuals with mental and substance use disorders, there are no published studies reporting training or competency related to treating CODs among these providers.
Using a statewide survey, we examined the extent to which social workers and alcohol and drug counselors in Minnesota are prepared to provide effective treatment for individuals with CODs by assessing providers’ (n=438) COD-related past training and practice experience.
Past Training
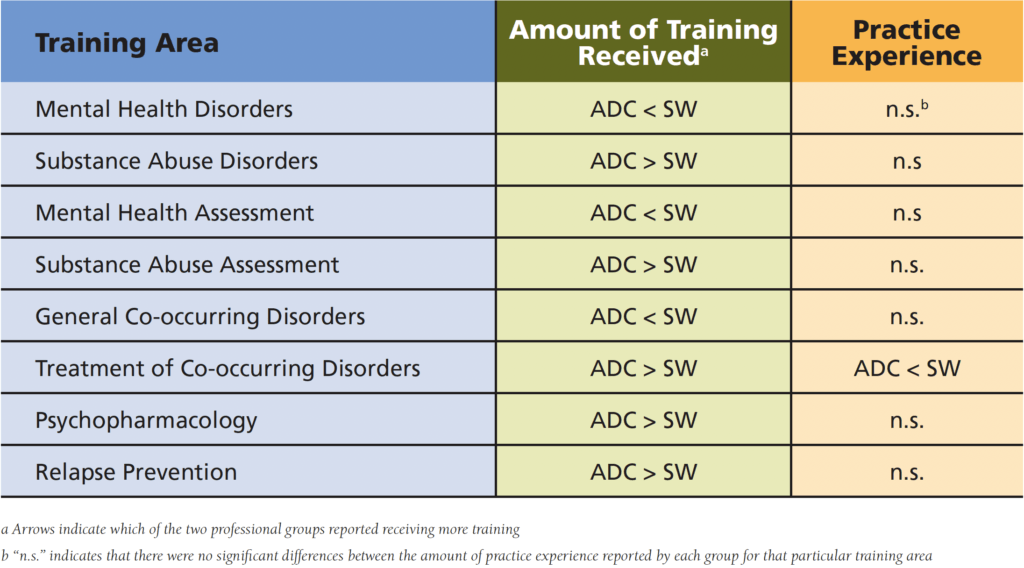
Not surprisingly, social workers reported receiving more training in mental health disorders than alcohol and drug counselors. The opposite was found for training in substance use disorders, with alcohol and drug counselors reporting more hours of training than social workers. Similar results were found for training in mental health and substance use assessment: social workers reported more training in mental health assessment while alcohol and drug counselors received more training in substance use assessment.
In terms of training specific to CODs, alcohol and drug counselors reported more hours of training in COD treatment, psychopharmacology, and relapse prevention. In contrast, social workers, reported receiving very little training on general CODs and in the treatment of CODs. These training differences may be due to the fact that alcohol and drug counselors in Minnesota who work in Rule 31 clinics (state licensed COD clinics) are required to demonstrate 8 COD-specific continuing education units (CEUs) each year for pro-gram license renewal. More recently, the state of Minnesota mandated 15 clock hours of COD training for all alcohol and drug counselors. The Minnesota Board of Behavioral Health and Therapy now also requires evidence of some academic training in CODs. Taken together, these requirements serve to ensure that alcohol and drug counselors obtain at least some ongoing COD training, while there is no such requirement in Minnesota for social workers who work with the same population.
Experience Working with Co-Occurring Disorders
Social workers reported more years of experience treat-ing clients with CODs compared with alcohol and drug counselors in this sample. However, practitioners from both groups who had less COD training were also less likely to have diagnosed or treated people with CODs in the past 12 months. Similarly, both social workers and alcohol and drug counselors with little training were most likely to report having never treated CODs during their professional careers. It is likely that a lack of COD-specific training will also hinder practitioners’ ability to appropriately recognize and diagnose COD among their clients.
Comparison of Social Workers’ and Alcohol and Drug Counselors’ COD Training and Practice Experience
Conclusions
From both a policy and practice perspective, there is a need for competent, well-trained professionals who can provide integrated treatment for CODs in a range of practice settings. In addition, the trend toward requiring certification for COD specialists currently seen in some states will likely continue. Social work and alcohol and drug counselor education programs, state licensing boards, and behavioral health agencies must encourage and support the training necessary to ensure that practitioners are prepared to provide competent and effective COD treatment. For example, State Boards of Social Work who oversee licensure of social workers could begin including a specified number of training hours in substance use and CODs similar to the requirements for alcohol and drug counselors. At the state policy level, programs that offer integrated COD treatment could be required to meet specific program standards for the training of staff in CODs. Educational institutions must also respond to this need by providing comprehensive training—from training infused in the core curricula of social work and alcohol and drug counselor programs to targeted CEU initiatives for practitioners in the field—that will serve new and experienced providers within this emerging practice area. Institutes focused on research and practice will be positioned to meet this growing need through evidence-based workforce training and development.
Findings from this survey suggest that tailored training and increased exposure to cross-discipline knowledge and communication is needed for social workers and alcohol and drug counselors to provide competent COD treatment. A new partnership between the Center for Practice Transformation and the Department of Human Services is leading the way to address this issue. Several Center initiatives are currently underway which provide workforce training, consultation, and evaluation to mental health and substance use professionals and agencies With the recent development of the IDDT rule (MN rule 9533), this is a ideal time to address workforce needs in COD training. Findings from the Minnesota Workforce Survey establish the increased need for training in CODs for both social workers and alcohol and drug counselors.
Publication Reference
Social Work Education: The International Journal
Volume 33, 2014 – Issue 5
Mental Health Quality Improvement Project for Assertive Community Treatment (ACT)
Funded by Minnesota Department of Human Services Behavioral Health DivisionDramatically high rates of mortality related to chronic health conditions among individuals with serious mental illness (SMI) have contributed to an increasing need for interventions to address this problem. Integrated Illness Management and Recovery (I-IMR) is an intervention that incorporates illness self-management strategies for mental and physical illnesses. This study piloted I-IMR using practitioners on Assertive Community Treatment (ACT) teams to investigate feasibility of I-IMR on at ACT team and outcomes associated with improvements in the physical and mental health of individuals with SMI.
I-IMR was found to be both feasible and effective with participants. Participants enrolled in I-IMR experienced reduced psychiatric and medical hospitalizations at post treatment, and improved psychiatric outcomes and general self-efficacy. There was no significant improvement in self-efficacy related to disease management.
Research Briefs
Disparities between Black and White Client Outcomes in Outpatient Treatment for Substance Use Disorder
The Center partnered with NUWAY® to investigate differences between Black and White clients at the time of their admission to services and at discharge. Results indicate that differences exist when clients are admitted to care and these differences are reduced at the time of discharge, showing that treatment services may play a positive role in reducing racial disparities.
Disparities between Indigenous American and White Client Outcomes in Outpatient Treatment for Substance Use Disorder
The Center partnered with NUWAY® to investigate differences between Indigenous American and White clients at the time of their admission to services and at discharge. Results indicate that the differences present when clients are admitted to treatment are not present at the time of discharge, indicating that treatment services are associated with reduction in disparities among Indigenous Americans with substance use disorders.
Predictors of Successful Discharge from Intensive Outpatient Treatment for Substance Use Disorders
The Center partnered with NUWAY® to investigate the association between participant characteristics and metrics of recovery at admission with successful completion of their treatment program. Results indicate that both demographic characteristics and recovery metrics are significant predictors of successful treatment completion.
Predictors of Client Dropout from Intensive Outpatient Substance Use Disorder Treatment
The Center partnered with NUWAY® to investigate the association between participant characteristics and metrics of recovery at admission and early dropouts from treatment. Results indicate that recovery metrics are better predictors of early dropout from SUD treatment.
Recovery Residence Populations: Differences in Characteristics of R.I.S.E. Participants and Self-Housed NUWAY® Clients
The Center and NUWAY® partnered to study the demographic differences between individuals who chose to participate in recovery housing and those who did not while receiving intensive outpatient care at NUWAY®. Results show women and people who are court ordered to treatment are choosing recovery housing at lower rates.
Recovery Residences and Improved Outcomes: The Association Between R.I.S.E. and Clinical Outcomes
The Center partnered with NUWAY® to investigate the association between living in recovery residences while attending intensive outpatient treatment and recovery outcomes. Results indicate that integrating recovery residences and intensive outpatient programming is associated with improved recovery outcomes.
The Effectiveness of Telehealth for Substance Use Disorder Treatment
The Center and NUWAY® partnered to investigate telehealth as a service delivery model in substance use disorder treatment. Results indicate a blend of in-person and telehealth services may deliver a flexible and ultimately effective experience for people receiving care.
Treatment of Co-occurring Mental Health and Substance Use Disorders: Preparedness of Social Workers and Alcohol and Drug Counselors in Minnesota
Of the 9.2 million Americans with co-occurring mental health and substance use disorders (CODs), only 44.4% received treatment for either mental illness or substance use disorder alone, while an even smaller minority (7.7%) received treatment for both (SAMHSA, 2012).
Integration of Mental Health and Primary Care: Barriers, Strategies, and Recommendations
Individuals with serious mental illness have a much shorter lifespan than the general population, with increased incidence of physical illness such as hypertension, diabetes, and respiratory disease (De Hert et al., 2011). To address the life expectancy gap between those with serious mental illness and the general population in Minnesota, the 10 x 10 initiative was started in 2008. The goal of this initiative is to increase the lifespan of individuals with serious mental illness by 10 years within 10 years.
Piloting Integrated Illness Management and Recovery with Assertive Community Treatment Teams: Targeting Physical Health in Persons with Serious Mental Illness
The Minnesota 10 by 10 initiative, led by the Minnesota Department of Human Services, has set a goal to increase the life expectancy of individuals with SMI by 10 years, in 10 years from its commencement in 2011 (Minnesota Department of Human Services, 2011). As part of the Minnesota 10 by 10 initiative, resources were developed to create opportunities for increasing discussion surrounding physical health screenings between health care providers, practitioners, clients, and their family members. The Center trained 10 ACT teams across Minnesota in the I-IMR model to examine the feasibility of an individualized intervention to address both mental and physical health needs. This Research Brief highlights the outcomes of the intervention.
Trainings Tailored to Your Team’s Needs
Talk with us about how we can build an evidence-based practice training plan for your team.